Musculoskeletal Cancer Care at Max Institute of Cancer Care
The Max Institute of Cancer Care (MICC) provides expert management for benign and malignant musculoskeletal tumors. Our Musculoskeletal / Orthopaedic Oncology Disease Management Group (DMG) is dedicated to delivering comprehensive care. We use a multidisciplinary approach involving molecular oncologists, pathologists, radiologists, onco-psychologists, nuclear medicine specialists, and various oncologists.
Personalized Treatment Plans
Each patient receives a tailored treatment plan through our multidisciplinary tumor board. Specialists collaborate to develop strategies that enhance survival and improve functional outcomes.
Surgical Interventions
We offer various surgical options for treating tumors:
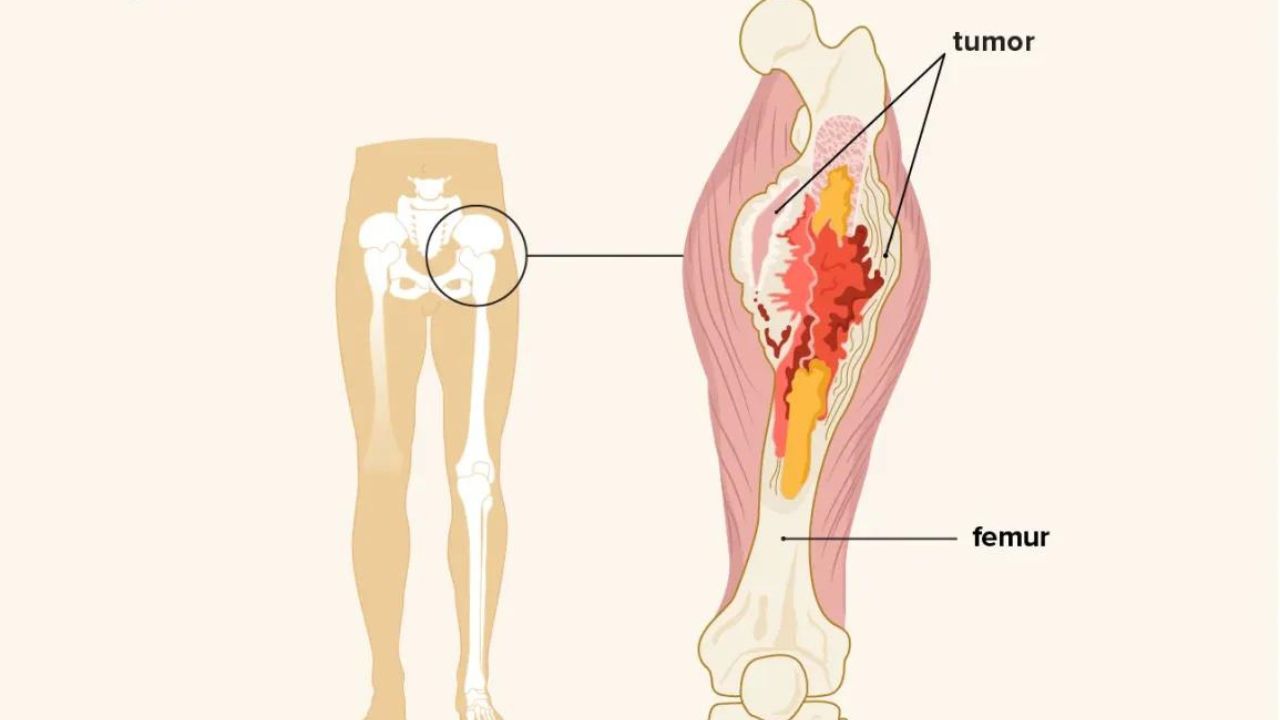
- Limb Salvage Surgery: This includes using prostheses, bone transplants, extracorporeal radiation therapy (ECRT), and cryosurgery for tumors like osteosarcoma and Ewing sarcoma.
- Soft Tissue Sarcoma Surgery: Our focus is on preserving limbs.
- Benign Tumor Treatment: Non-surgical methods such as sclerotherapy and radiofrequency ablation are used for conditions like osteoid osteoma and simple bone cysts.
- Metastatic Bone Disease: Treatments include adjuvant fixations and minimally invasive techniques like vertebroplasty and balloon kyphoplasty for spine tumors.
Medical and Radiation Oncology
- Chemotherapy: We use chemotherapy for both bone and soft tissue sarcomas. This includes palliative care for advanced stages and high-dose chemotherapy with stem cell transplantation when needed.
- Radiation Therapy: We apply radiation therapy before, during, and after surgery based on the case. Techniques include high-dose precision radiation therapy, interstitial brachytherapy, and ECRT to effectively target tumors while minimizing long-term side effects.
Advanced Techniques and Technologies
At MICC, we utilize advanced radiation methods such as intensity-modulated radiation therapy (IMRT), image-guided radiation therapy (IGRT), and stereotactic body radiation therapy (SBRT). These techniques help precisely target tumors and reduce damage to surrounding tissues.
Our goal is to offer personalized, evidence-based care using the latest technologies and multidisciplinary expertise. This ensures the best possible outcomes for our patients.